
It’s 8:32 am and there’s already a growing line at the dispensary. A mum is waiting for an Amoxycillin script for her baby, a man wants a flu shot before work, and an older couple is here for a blood pressure check. By 10.00 am, scripts are piling up, the phone keeps ringing, and a scheduled MedsCheck has been pushed back – yet again.
This scene is painfully familiar to many community pharmacists. It reflects workflows designed for a time when pharmacy was mostly about dispensing. Expanded scope of practice and rising patient demand now sit alongside workforce shortages, financial pressure, and administrative burden. When workflows have not evolved, these pressures collide, and the whole system heaves under the weight.
In this context, workflow integration isn’t optional. It requires deliberately redesigning how work flows through the pharmacy – from role delegation and training to using existing digital tools to protect clinical time. When done well, it allows pharmacies to deliver more services without overwhelming staff or compromising care.
What is integration?
In a pharmacy, workflow integration means organising work so dispensing, services, staff roles, and technology fit together, rather than constantly interrupting each other.
An integrated workflow allows routine tasks to move through the pharmacy without the pharmacist needing to step in each time. Support staff manage defined steps, systems support the process, and the pharmacist is involved where clinical judgement is actually needed.
But workflow integration is often misunderstood. This is what it is not:
- Buying new software and hoping it fixes the problem. If processes and roles stay the same, technology usually adds work instead of reducing it.
- Rigid flows which remove professional judgement. Effective workflows structure routine tasks so pharmacists have more time to think clinically, not less.
Deliberate design
Traditional pharmacy workflows have largely been built around the dispensing cycle. As clinical services expanded, they were often added in response to funding or patient demand, rather than designed into everyday work. Over time, this has created workflows where tasks accumulate, but the way work moves through the pharmacy remains largely unchanged, a concerning pattern commonly found in healthcare workflow and quality improvement literature (World Health Organization, 2010).
In many community pharmacies, this means pharmacists are expected to manage dispensing, interruptions and clinical services all at the same time. These workflows rely heavily on individual effort and memory to keep things moving, which becomes difficult to sustain in a busy environment and is recognised as a contributor to error risk in primary care settings (Reason, 2000).
Traditional workflows
In a traditional model, service delivery is usually reactive. Bookings are jotted down informally, patients are identified for services on the spot, and documentation is completed when time allows. Handover between staff or shifts can be inconsistent, particularly on busy days. Studies examining service delivery in community pharmacy have shown reliance on informal processes increases variability and makes care less reliable as workload increases (Chui et al., 2011). While this approach may work when demand is low, it becomes increasingly fragile as work piles up.
Walk in requests
Let’s think about a busy suburban pharmacy on a typical morning. Prescriptions build steadily alongside walk-in requests. A patient asks for a blood pressure check, which the pharmacist agrees to fit in shortly, while another patient requests an absence from work certificate, and the booking is jotted down in the diary (or in the online calendar if you are really fancy).
As dispensing demand increases, the pharmacist is interrupted repeatedly. The blood pressure check is delayed, the absence from work certificate is delayed more than once, and documentation is completed retrospectively. A shift change occurs without a clear handover, and a follow-up referral is missed. While no serious incident occurs, the risk increases with each passing day.
Integrated workflow
In the same pharmacy, with the same staff and patient demand, an integrated workflow looks very different. The day starts with a service schedule supported by an appointment system managed by a trained assistant. Patients requesting services are triaged at the counter using simple prompts, and eligible services are booked into protected consultation times, aligning with recommended approaches to service planning in community pharmacy (Pharmaceutical Society of Australia, 2020).
Assistants manage service intake and preparation, allowing the pharmacist to conduct consultations with fewer interruptions. Documentation is completed as services occur, and follow-up actions are clearly assigned. This approach supports continuity of care and reduces reliance on individual memory, both of which are recognised contributors to safer practice (Reason, 2000).
Why the difference matters
The difference between these models comes down to how work is designed. Traditional workflows depend on individuals holding everything together under pressure, which makes service delivery inconsistent and harder to sustain. Integrated workflows shift that load onto shared systems, clearer roles, and better visibility of capacity – principles commonly reflected in quality and safety frameworks (Australian Commission on Safety and Quality in Health Care, 2021).
Integrated workflows do not happen by accident. They require deliberate design and are often supported – but not created – by digital tools. Understanding how technology can support these workflows is an important step in moving from traditional practice to a more integrated model of care.
Digital health integration
Most Australian community pharmacies already use multiple digital systems. The challenge is not access to technology; it’s how well those tools are aligned with day-to-day workflow. Without deliberate design, digital systems show relevant information but fail to translate it into consistent action.
Dispensing systems provide insight into medication histories and repeat use. Service platforms support eligibility checking, service delivery, and follow-up, while secure messaging and My Health Record support continuity of care. On their own, these tools increase productivity in siloes, and existing digital integrations between various platforms make the work easier. But value is created only when they are embedded into how work actually happens in the pharmacy (World Health Organization, 2010).
Why digital tools often fall short
Even in well-resourced pharmacies, a small number of issues commonly limit effective digital use.
As systems accumulate, staff move between multiple platforms without a clear sense of priority. When tools are layered onto existing processes rather than integrated into them, cognitive load increases and informal workarounds emerge. Documentation and follow-up may sit outside the dispensing workflow, requiring information to be entered more than once and increasing the risk of missed handover (Australian Commission on Safety and Quality in Health Care, 2021).
Change fatigue also plays a role. When new tools or processes are introduced too quickly, staff struggle to embed them into their workflows. Adoption is delayed not because the technology lacks value, but because teams are not given time to get used to them. Evidence from healthcare change literature shows that pacing and sequencing are critical to sustained adoption (World Health Organization, 2010).
In practice, digital health integration in pharmacy is not about adopting new platforms. For most pharmacies, that’s already happened. It is about aligning existing systems with workflows that support safety, staff wellbeing, and sustainable service delivery.
Solution 1 Proactive and reactive digital workflows
A practical starting point for workflow integration is being clear about how patients are identified for services. In many pharmacies, this still happens in an ad hoc way, often relying on individual judgment at the counter. Research into community pharmacy workflow shows that this variability leads to unreliable outcomes, particularly as workload increases (Chui et al., 2011). Integrated models address this by using two complementary pathways: proactive and reactive workflows.
Proactive workflows identify service opportunities before pressure builds. In practice, this involves reviewing service dashboards or dispensing data at set intervals to identify patients due for follow-up services, vaccinations, or reviews. Assistants can then initiate booking conversations, allowing services to be planned into available consultation time rather than competing with dispensing demand. This approach fits with established principles of healthcare workflow design (World Health Organization, 2010).
Reactive workflows operate during routine dispensing interactions. Medication context can signal potential service needs, and with appropriate training, assistants can confirm eligibility and offer bookings rather than attempting to deliver services immediately. Structured prompts reduce reliance on memory and help maintain safety during busy periods (Australian Commission on Safety and Quality in Health Care, 2021).
When both pathways are used together, service identification becomes consistent rather than opportunistic. This reduces missed services and allows demand to be managed deliberately, supporting both patient care and business sustainability.
Solution 2 Scheduling and follow-up (day-to-day control)
Identifying services is only effective if delivery is actively controlled on the day. Without deliberate scheduling, services are often delayed or abandoned. Protecting clinical time through defined consultation slots and visible booking systems allows demand to be matched to capacity and reduces disruption to dispensing flow (Australian Commission on Safety and Quality in Health Care, 2021).
In practice, this means services are not delivered whenever time appears. They are booked into known consultation blocks that are visible to the whole team and managed by support staff. This prevents pharmacists from needing to juggle dispensing and consultations simultaneously and reduces task switching on busy days.
Documentation and follow-up are part of this same operational control. When left until later, they create rework, missed referrals, and poor handover. When completed as the service occurs, they support continuity of care and repeat engagement. Digital tools that prompt real-time documentation and follow-up reduce reliance on memory and help ensure the service is completed end-to-end, not just delivered.
Solution 3 Implementing digital integration incrementally
Even well-designed workflows fail if too much change is introduced at once. A common reason digital integration stalls is change fatigue rather than a lack of capability. Pharmacies that integrate successfully tend to sequence changes deliberately instead of attempting full redesign in one step.
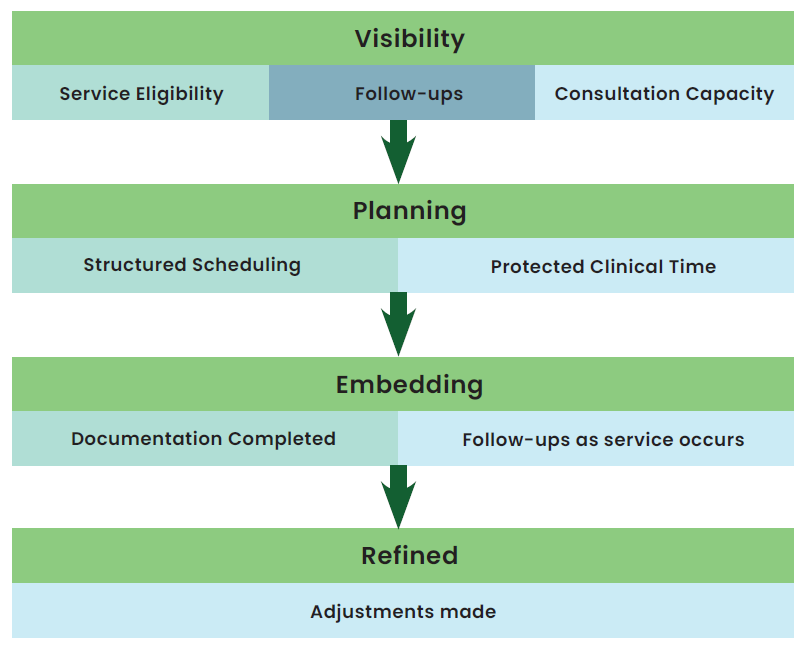
The first stage is visibility. Service eligibility, follow-ups, and consultation capacity are made visible to the team, reducing reliance on individual memory. The next stage is planning, where that visibility is used to introduce structured scheduling and protected clinical time. The third stage is embedding, where documentation and follow-up are built into the workflow so they are completed as services occur. Finally, workflows are refined over time, with adjustments to service mix, handover processes, and staff roles.
Digital integration is not about adopting new platforms. It is about aligning existing systems with how work actually happens in the pharmacy. By sequencing changes rather than layering them, teams are more likely to adopt new workflows consistently and sustain them over time (World Health Organization, 2010).
Optimising staff roles
Effective workflow integration in community pharmacy depends on how clearly work is divided and handed between staff. While technology can support this, the day-to-day success of any workflow depends on people. In particular, pharmacy assistants play a critical role in whether services are delivered consistently.
Optimising staff roles is not about asking assistants to do more. It is about deciding, deliberately, which parts of service delivery require clinical judgement and which do not. In many pharmacies, pharmacists continue to manage tasks that could easily be handled by support staff. This creates bottlenecks and limits service capacity. Redesigning roles so assistants manage these non-clinical steps allows pharmacists to focus on assessment, decision-making, and patient care (Pharmaceutical Society of Australia, 2020).
Defining ownership
A common problem in traditional workflows is unclear ownership. Tasks are completed “when someone has time,” leading to delays, duplication, and missed follow-up. Clear ownership reduces reliance on memory and constant task-switching, both of which are known contributors to error in busy healthcare environments (World Health Organization, 2010; Reason, 2000).
Integrated workflows address this by clearly assigning responsibility at each stage of service delivery. In practice, assistants can reliably own the front end of the workflow. This includes identifying potential service opportunities using structured prompts, offering services during routine interactions, managing bookings into defined consultation times, preparing intake information before the pharmacist sees the patient, and coordinating follow-up after consultations. This already occurs informally in many pharmacies; integration simply formalises it. With greater role clarity and lower stress, teams are more resilient (Pharmaceutical Society of Australia, 2020).
Redesigning staff roles
Once proactive and reactive workflows are established, the key change is how responsibility is distributed across the team.
In integrated pharmacies, service identification is no longer a pharmacist-led task. Assistants are responsible for running both proactive and reactive pathways, using structured prompts and eligibility lists to initiate bookings. This shifts service identification away from individual judgement and reduces the need for pharmacists to monitor opportunities while dispensing.
The pharmacist’s role moves downstream. Rather than identifying who is eligible for a service, pharmacists focus on clinical assessment, consultation delivery, and decision-making once patients are booked. Clear escalation points ensure that clinical questions are addressed without disrupting dispensing or scheduled consultations.
This role separation reduces interruptions and makes service delivery less dependent on who happens to be working or how busy the dispensary is. Research shows that when service identification is structured and team-based, variability in delivery decreases and workflows become more reliable (Chui et al., 2011).
Setting boundaries
Effective delegation depends on clear boundaries. Assistants should know exactly where their role ends and when to escalate to the pharmacist. This is best achieved through simple decision rules rather than lengthy protocols.
For example, assistants may confirm eligibility and manage bookings, but any clinical assessment, medication changes, or patient concerns outside defined criteria are referred immediately to the pharmacist. Though this is often what happens in the pharmacy context anyway, clear escalation pathways protect patient safety and increase assistant confidence, reducing hesitation and inconsistent practice (Australian Commission on Safety and Quality in Health Care, 2021).
Upskilling assistants
Upskilling works best when it is narrow, staged, and linked to specific workflows. Attempting to expand roles across multiple services at once often leads to confusion and resistance. A more effective approach is to embed one service workflow at a time.
For example, assistants may first be trained to manage vaccination bookings, intake, and follow-up. Once that workflow is stable, the same structure can be extended to medication reviews or health checks. Training should include clear scripts, supervised practice during early implementation, and regular feedback focused on workflow quality rather than speed.
Evidence from community pharmacy studies suggests that task-specific training, reinforced through daily practice, leads to more consistent performance than broad role descriptions alone (Chui et al., 2011).
Managing patient flow
Patient-centred care in community pharmacy is shaped as much by flow as by communication. Walk-in access remains a defining feature, but unmanaged walk-ins are a major source of interruption.
Integrated workflows use counter triage to determine urgency and next steps. Assistants ask a small number of standard questions, check eligibility, and offer clear options: immediate service if appropriate, a scheduled time, or referral. Patients are generally accepting of scheduled care when wait times and processes are explained clearly.
This approach reduces constant task-switching and protects clinical time, both of which are linked to safer dispensing and more reliable service delivery (Reason, 2000).
Multidisciplinary care
Well-designed workflows support collaboration beyond the pharmacy by making communication routine rather than optional. Consistent documentation, clear referral triggers, and structured handover processes reduce reliance on individual follow-up and improve the reliability of information shared with GPs, nurses, and other health professionals.
In practice, this starts with defining when a referral is required and who initiates it. Integrated workflows use agreed triggers, such as specific medication changes, clinical findings, or unmet monitoring needs; so referrals are not dependent on individual judgement or memory. Assistants can prepare referral documentation as part of the service workflow, allowing pharmacists to focus on clinical assessment and decision-making.
Follow-up is equally important. When responsibility for tracking referrals and responses is assigned, pharmacies are better able to close the loop on care. This may include maintaining a visible follow-up list, setting clear timeframes for review, and confirming outcomes during subsequent patient interactions. These steps support continuity of care and reduce the risk of recommendations being missed or acted on late.
As pharmacists take on expanded clinical roles, reliable information sharing becomes central to safe practice. Integrated workflows ensure that communication with external providers is timely, consistent, and embedded into daily operations, rather than treated as an extra task. This strengthens the pharmacy’s role within the broader healthcare team and supports coordinated, patient-centred care (Australian Commission on Safety and Quality in Health Care, 2021).
Conclusion
Workflow integration in community pharmacy is not about efficiency. It is about sustainability of care, of staff, and of the business. As pharmacists take on broader clinical responsibilities, poorly designed workflows create risk. Well-designed workflows reduce it. Integrated workflows do not require new technology. They require clear role design, managed patient flow, and systems that support consistent practice instead of individual memory. Workflow integration does not happen by accident. It requires deliberate design and ongoing leadership. For community pharmacies, it is the foundation of modern, sustainable practice.
Australia
Accreditation Number: A2603AUP1
Accreditation Expiry: 31/12/2027
Pharmacist Competencies: 1.1, 1.6, 4.3, 4.4, 4.5, 4.6, 4.7
New Zealand
This article aims to equip you with the tools necessary to meet recertification requirements and actively contribute to the growth of your professional knowledge and skills.
Effectively contribute to your annual recertification by utilising this content to document diverse learning activities, regardless of whether this topic was included in your professional development plan.
References
- Australian Commission on Safety and Quality in Health Care. (2021). Communicating for safety.https://www.safetyandquality.gov.au
- Chui, M. A., Mott, D. A., & Maxwell, L. (2011). A qualitative assessment of workflow in community pharmacies. Research in Social and Administrative Pharmacy, 7(4), 364–377.
- Pharmaceutical Society of Australia. (2020). Community pharmacy service delivery guidelines. PSA.
- Reason, J. (2000).Human error: Models and management.BMJ, 320(7237), 768–770. https://doi.org/10.1136/bmj.320.7237.768
- World Health Organization. (2010). Human factors in patient safety: Review of topics and tools. WHO Press.









